
A Person Within the Ecosystem
Tamaoka:
Could you tell us about the clinical practice and research you are involved in at Osaka City General Hospital?
Morita:
Osaka City General Hospital is the largest public hospital in Osaka City, located in the northern part of the city, with 46 clinical departments and 1,063 beds. It is designated as both a Category I and Category II infectious disease medical institution, meaning that we are equipped to manage patients with highly hazardous infectious diseases, including viral hemorrhagic fevers such as Ebola.
Our infectious diseases practice consists of three major pillars.
The first is the management of common infectious diseases, including pneumonia, urinary tract infections, cholangitis, enteritis, influenza, and COVID-19. During the COVID-19 pandemic, we began accepting patients in January 2020 and played a central role in the response across Osaka Prefecture. As I will mention later, infection prevention and control within the hospital is also an important part of our work.
The second pillar is the management of sexually transmitted infections, particularly HIV infection, including the care of patients living with AIDS. We also place considerable emphasis on the diagnosis and treatment of syphilis. In collaboration with the departments of obstetrics and neonatology, we manage pregnancies complicated by syphilis as well as infants with congenital syphilis.
The third pillar is travel-related infectious diseases. As a member of the national research group on tropical disease therapeutics, I am involved in the management of patients with severe Plasmodium falciparum malaria. We also specialize in the diagnosis and treatment of a wide range of parasitic diseases and arthropod-borne infections. Opportunities to manage tick-borne diseases have increased in recent years, and we have recently treated patients with severe fever with thrombocytopenia syndrome (SFTS), Japanese spotted fever, scrub typhus, and African tick-bite fever. In addition, we care for patients with tuberculosis and nontuberculous mycobacterial disease, the latter of which has been steadily increasing in prevalence.
Our research is closely linked to our extensive clinical experience. We collaborate with Osaka Metropolitan University, Osaka University, the Osaka Institute of Public Health, the Japan Institute for Health Security, the Research Institute of Tuberculosis, and other institutions to conduct research on HIV, syphilis, malaria, mpox virus, arboviruses, nontuberculous mycobacteria, and other infectious diseases.
Tamaoka:
What inspired you to specialize in infectious diseases?
Morita:
When I first became a physician, I was actually more interested in basic research than in clinical medicine.
I joined the Department of Parasitology at Osaka City University (now Osaka Metropolitan University), where Professor Akira Kaneko was chair at the time. Professor Kaneko is a malaria researcher who led malaria control projects in Vanuatu and Kenya, and his work had a tremendous influence on me.
Another faculty member, Professor Isao Kimata, taught me the fundamentals of parasitology, particularly parasite morphology. Later, Professor Yasutoshi Kido, who now chairs the department, introduced me to the future directions of parasitology and infectious diseases. Dr. Wataru Kagaya, who is currently at Nagasaki University, showed me the excitement of research and generously mentored me on many occasions.
Learning in such an inspiring environment led me to aspire to conduct research on parasitic and tropical diseases, which naturally drew me toward the field of infectious diseases.
I’ve also loved living creatures since childhood. During junior high and high school, I participated in the Junior Natural History Club at the Osaka Museum of Natural History, where we went out to observe birds, insects, and plants.
Within an ecosystem, countless organisms interact with one another, and these relationships are never one-sided. As I studied parasitology in medical school, I came to realize that humans are simply one species embedded within this ecosystem.
Even the pathogenic microorganisms that often cause us suffering are themselves struggling to survive, just as we are. I find it deeply fascinating to understand these organisms and confront them directly in order to restore patients’ health. That, to me, is what makes infectious disease medicine such an attractive field.
Tamaoka:
What do you find most rewarding about working as an infectious disease physician?
Morita:
Medicine is, in many ways, a contest between humans and pathogenic microorganisms. As physicians, we stand on the patient’s side, fighting alongside them against the pathogens causing their illness. Seeing patients regain their health through that process is incredibly rewarding.
I see antimicrobial agents as an assist rather than the decisive player. While they are essential tools that help combat pathogens, it is ultimately the patient’s own immune system that brings the infection under control. Helping optimize a patient’s overall condition so that their immune system can overcome the infection—and providing antimicrobial therapy as that crucial assist—is one of the most fulfilling aspects of my work.
Another rewarding aspect is that many infectious diseases are transmissible from person to person. Successfully treating one patient’s infection is therefore not only beneficial for that individual but also has important public health implications for protecting others.
The COVID-19 pandemic reinforced this perspective. By working together with public health authorities, we can protect communities. Likewise, through basic research, we can contribute to improving people’s health on a broader scale.
One of the greatest attractions of infectious disease medicine is that it offers so many different avenues through which we can make a meaningful impact on society.
Tamaoka:
On the other hand, what do you find most challenging about being an infectious disease physician?
Morita:
Patients are literally fighting for their lives—but so are the pathogens.
As pathogens replicate within the human body, they continuously acquire genetic mutations. Under the selective pressures imposed by the host immune system and antimicrobial agents, more resilient variants emerge and survive. I am constantly impressed by both the speed and sophistication of this evolutionary process, while at the same time finding it one of the greatest challenges in infectious disease medicine.
Another challenge, though certainly not one unique to infectious diseases, is that medicine ultimately cares for people. Things do not always unfold as we hope.
When I put myself in my patients’ shoes, I understand that it is not always possible for them to follow every medical recommendation exactly as instructed. People’s decisions are shaped by many factors—their living circumstances, psychological burdens, financial constraints, cultural backgrounds, dependence on others, or social isolation. Under such circumstances, patients cannot always choose what is medically considered the best course of action.
That is why, rather than blaming patients for their behavior, I believe it is essential to understand the context behind their decisions and provide care accordingly. I don’t necessarily see this as a difficulty; rather, it is something profoundly human, and one of the reasons I genuinely enjoy practicing medicine.
Tamaoka:
How are collaboration and decision-making carried out within the hospital?
Morita:
One of the important responsibilities of an infectious disease physician is infection prevention and control within the hospital.
As members of the Antimicrobial Stewardship Team (AST) and the Infection Control Team (ICT), we work closely with professionals from many different departments. These teams are sometimes perceived as “the people who come and tell everyone what to do,” but I don’t see it that way. I believe we are part of the same team as the physicians and healthcare professionals we work with, all striving toward the same goal.
For example, there are situations in which a physician wishes to prescribe a broad-spectrum antibiotic, while the AST recommends a more microbiologically appropriate agent to minimize the development of antimicrobial resistance. In such cases, our opinions may differ.
Finding the best compromise—one that balances both perspectives in the patient’s best interest—is often challenging. It requires strong communication skills and, above all, trust that has been built through everyday collaboration.
To achieve this, I don’t think our work should be limited to phone calls or comments in the electronic medical record. Whenever possible, it is important to meet colleagues in person, discuss the case together, and even visit the patient together at the bedside. These face-to-face conversations often lead to deeper and more productive discussions.
Likewise, I never hesitate to leave the bedside and visit the microbiology laboratory, the pharmacy department, or other areas of the hospital whenever necessary.
Ultimately, everyone working in healthcare shares the same goal: improving the lives of our patients. Although we sometimes engage in passionate debates, being able to collaborate with colleagues who all share that commitment is something I consider a true privilege.
Globalization and Infectious Disease Practice
Tamaoka:
I understand that Osaka City General Hospital also manages travel-related infectious diseases. How do you view the current situation regarding infectious diseases, including imported infections, in Osaka?
Morita:
Now that the COVID-19 pandemic has subsided, many Japanese people are once again traveling abroad, while increasing numbers of international visitors are coming to Japan. In addition, many people from Southeast and South Asian countries, such as Vietnam, Myanmar, and Nepal, have come to Japan to work.
As sanitary conditions have improved in many low- and middle-income countries, imported tropical diseases are less frequently encountered than in the past. However, new infectious diseases continue to emerge, and international travel and migration are expected to become even more active in the years ahead. Therefore, we must remain vigilant.
Osaka has historically had one of the highest tuberculosis burdens in Japan, and we are seeing a growing number of tuberculosis cases among foreign workers and international students. Likewise, the number of non-Japanese patients living with HIV has also been increasing. These are important issues that require thoughtful and sustained attention.
Tamaoka:
When caring for international patients, what do you consider particularly important? Are there any challenges that stand out?
Morita:
When treating Japanese patients, we can often form a general understanding of the social and cultural environment in which they have lived. With international patients, however, this is not always possible.
It is important to imagine the life each patient has led and to provide care with as much consideration as possible for their cultural, religious, political, and ethnic backgrounds.
Communication presents another major challenge. When patients cannot communicate effectively in either Japanese or English, we rely on various interpretation services. While telephone and tablet-based interpretation are convenient, they often fail to convey subtle nuances, such as facial expressions and the atmosphere of the conversation. Whenever possible, we therefore prefer to have professional interpreters present in person during consultations.
Fortunately, there is a local non-profit organization called CHARM, located near our hospital, that provides outstanding support for foreign residents. We frequently collaborate with them.
I remember one particularly memorable case involving a Vietnamese technical intern trainee in his thirties. He had become too ill to continue working, lost his residence status, and was admitted to our hospital with suspected tuberculosis. After further evaluation, however, he was diagnosed with Ewing sarcoma, a malignant bone and soft tissue tumor.
Breaking the news of a cancer diagnosis is never easy, even for Japanese patients. In his case, it was especially challenging because he spoke neither Japanese nor English.
Fortunately, CHARM arranged for a professional medical interpreter, enabling us to explain his diagnosis and treatment options carefully through interpretation.
Ultimately, he wished to return to Vietnam to receive treatment near his family. Together with local government officials, we accompanied him as far as Vietnam to ensure a safe transfer of care.
Being able to reunite him with his family was a deeply moving experience for all of us.
Japan’s Role and Future Potential in Tropical Medicine
Tamaoka:
The Student Committee of the Japanese Society of Tropical Medicine brings together students who are interested in tropical medicine. In your view, how can Japan contribute to this field?
Morita:
Japan succeeded in eliminating schistosomiasis relatively early, and I believe this achievement is a legacy of which we can be truly proud. It was made possible through the dedicated efforts of everyone involved in public health—not only government officials, but also researchers and, above all, local communities.
I believe Japan can contribute by sharing both the scientific and technological expertise it has cultivated over many years and the collaborative strategies through which governments, researchers, and communities work together to improve public health. These experiences may prove valuable in regions where infectious disease control remains challenging.
Today, tropical medicine and global health encompass much more than infectious diseases alone. Noncommunicable diseases (NCDs) have also become major health concerns. While many tropical regions continue to face challenges related to infectious diseases, nutrition, and maternal and child health, they are simultaneously experiencing increasing burdens from diabetes, hypertension, cardiovascular diseases, chronic kidney disease, and cancer.
Rather than viewing infectious diseases and NCDs as separate issues, we need to consider them within a broader context that includes socioeconomic conditions, access to healthcare, living environments, and urbanization. I believe Japan has much to contribute by promoting such integrated approaches to health.
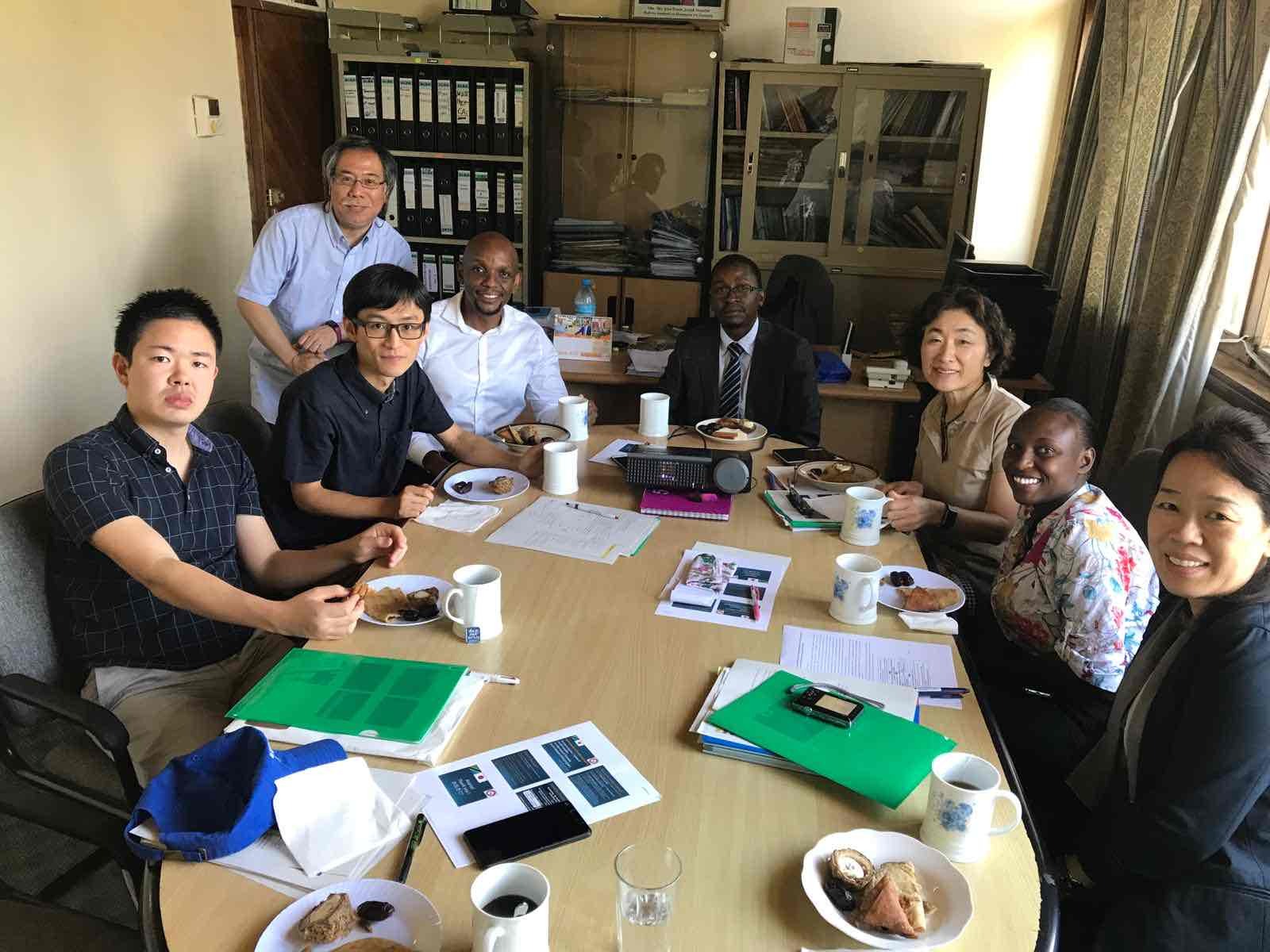
Most importantly, however, these efforts should never be one-sided. We must work collaboratively with local researchers, healthcare professionals, and communities, learning from one another throughout the process.
Having visited countries such as Kenya, Tanzania, Thailand, and Vietnam, I have come to feel that Japan—and Japanese people in general—are highly trusted by many of our international partners. The opportunity to address infectious diseases on the foundation of that trust is one of Japan’s greatest and most valuable strengths.
Tamaoka:
How do you think the role of tropical infectious diseases in Japan will evolve in the future?
Morita:
From a global perspective, I believe the importance of tropical regions will continue to grow.
Many tropical countries are part of what is often referred to as the Global South, and their influence is increasing in terms of population, economic development, culture, and academic activity. At the same time, these regions face complex and overlapping health challenges—not only infectious diseases, but also NCDs, urbanization, climate change, limited access to healthcare, and health inequities.
As more people travel from Japan to tropical regions and more people from tropical regions come to Japan, we are likely to encounter tropical infectious diseases more frequently in clinical practice. We may also need to respond to occasional localized outbreaks within Japan.
On the other hand, I believe that the burden of many tropical infectious diseases will gradually decline as sanitation and public health conditions continue to improve. In fact, compared with two decades ago, we now see far fewer malaria patients returning from Southeast Asia.
However, mosquito-borne viral diseases such as dengue are unlikely to be eradicated so easily. With diseases like these, an important concept is that they can impose a substantial socioeconomic burden even when their case-fatality rates are relatively low.
This is precisely why neglected tropical diseases (NTDs) should never be neglected. They deserve the attention and commitment that their name unfortunately suggests they have long lacked.
Tamaoka:
What are your personal goals and aspirations for the future?
Morita:
I hope to accomplish something that only I can achieve.
Helping the patients in front of me is deeply rewarding, and I feel fortunate to be able to do so. But if possible, I would like to contribute to improving the health of entire populations.
To achieve that, I hope to make discoveries that challenge and reshape our current scientific understanding.
Beyond that, I also hope to help create a world in which humans and countless other living organisms can coexist sustainably. Perhaps that goal extends beyond what an infectious disease specialist alone can accomplish—but it is something I continue to aspire to.
Tamaoka:
Finally, do you have a message for the members of the Student Committee of the Japanese Society of Tropical Medicine?
Morita:
My advice is simple: don’t limit yourself.
I know students are busy, but you also have a degree of freedom in how you spend your time. Whether or not it is directly related to medicine, I encourage you to experience as many different things as possible.
Rather than simply letting your student years pass by, immerse yourself wholeheartedly in something that truly interests you.
Universities offer an exceptional environment, surrounded by researchers with diverse expertise. If you ask them about their work, most will be delighted to share it with you. Some may even invite you to join them in fieldwork or attend academic conferences. Those experiences can be truly invaluable.
From the perspective of tropical medicine, I especially encourage you to travel—whether abroad or within Japan. Meet people, talk with them, and experience firsthand the incredible diversity of cultures, lifestyles, and ways of thinking.
Wherever you go in the world, you will find people striving to live their lives to the fullest. I hope you will discover both the similarities that connect us and the differences that make each community unique.
Those experiences will undoubtedly enrich not only your understanding of tropical medicine, but also your life itself.
Profile of Interview Participants
Dr. Ryo Morita
Dr. Ryo Morita is an infectious disease physician at Osaka City General Hospital. After graduating from the Faculty of Medicine at Osaka City University (now Osaka Metropolitan University), he completed his postgraduate clinical training at Rinku General Medical Center and Osaka City University Hospital. During medical school, he developed a strong interest in infectious diseases through his work in the Department of Parasitology. He currently provides comprehensive clinical care for a wide range of infectious diseases, from common community-acquired infections to imported and tropical diseases. His hobbies include traveling, mountaineering, fishing, and birdwatching.
Yuki Tamaoka
Yuki Tamaoka is a second-year medical student at the Faculty of Medicine, Kumamoto University. Originally from Matsuyama, Ehime Prefecture, she graduated from the St. Luke’s International University College of Nursing in 2024 before entering Kumamoto University to pursue a medical degree. Having spent her junior and senior high school years overseas, she developed a strong interest in providing healthcare for patients from diverse cultural backgrounds and in improving healthcare support for international residents in Japan. Her academic interests include infectious diseases and public health. She aspires to become a physician engaged in both clinical practice and clinical research while serving as a bridge between medicine and society.

