
A Shift to Tropical Medicine and the Challenges Ahead
Sano:
You are in charge of the “Learning Tropical Infectious Diseases through Clinical Cases” session at the Japanese Society of Tropical Medicine. When did you decide to pursue tropical medicine?
Nakamura:
After graduating from Miyazaki Medical College, I initially spent a year in obstetrics and gynecology. But once I was in it, it didn’t quite feel right. I was on the swimming team during med school, and my advisor, Professor Yukifumi Nawa, took good care of me—I’d often drop by the parasitology department even as a student. When I decided to leave obstetrics and gynecology, I was offered a position as an assistant in the parasitology department, as they happened to have an opening.
At that time, I wasn’t thinking of “tropical medicine” yet. I was researching the mechanisms of intestinal parasite elimination and doing immune diagnostics for parasitic diseases. But when I was thinking about what to do after getting my degree, I began to wonder: all these cross-reactions we struggled with in immune diagnostics—what do they actually look like in real patients? That question led me to Bokutoh Hospital.
Dr. Kenji Onishi, a researcher of echinococcosis and a graduate of Asahikawa Medical University, was the head of infectious diseases at Bokutoh. He used to give special lectures every year at Miyazaki Medical College, and I felt I had no choice but to rely on him if I wanted to study clinical medicine. That’s where my clinical path began.
For the first ten years after graduation, I was mostly in research, so during my clinical rotation at Bokutoh, I trained alongside newly graduated residents in internal medicine.
Sano:
So you actually started in obstetrics and gynecology!
Nakamura:
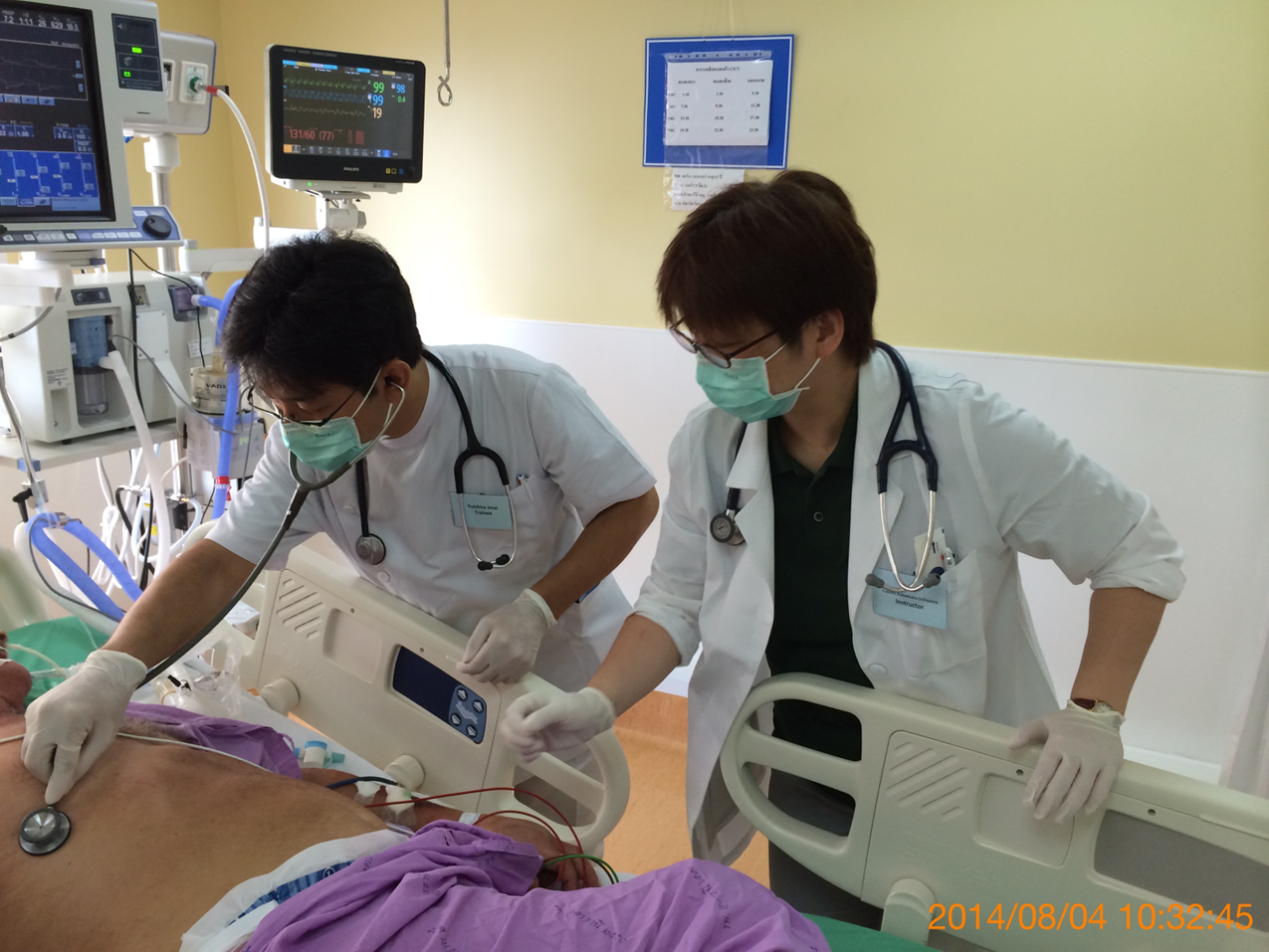
Yes, that’s right. As for when I first got involved in tropical medicine—well, I was at Bokutoh Hospital from 2006 to 2012. During that time, Professor Kazunori Oishi from the Research Institute for Microbial Diseases at Osaka University launched the Thailand-Myanmar Tropical Medicine Training Program, and I was able to participate as part of the second cohort.
Before that, I also joined a training program in Thailand organized by Nagasaki University. I had already seen patients with malaria and tapeworm infections at Bokutoh, but that training trip was my first actual visit to a tropical region.
The Gap Between Japan and Endemic Settings
Sano:
What were some of the challenges you faced once you became involved in tropical medicine?
Nakamura:
I felt there was a clear difference between tropical diseases as seen in endemic countries and as seen in Japan. For example, when I give lectures, I always say this: in Japan, we’re taught that the three classical signs of malaria are fever, splenomegaly, and anemia. But in reality, when a Japanese patient gets malaria for the first time, yes—they have a fever, and maybe slight splenomegaly that you’d only pick up on ultrasound. But anemia? No. In fact, they’re often dehydrated and hemoconcentrated.
In endemic areas, patients’ clinical presentations are shaped by repeated exposure, but in non-endemic settings like Japan, each case stands alone. That distinction really matters.
When you conduct tropical medicine fieldwork and aim to implement an intervention, you usually do so at the population level—thinking in terms of public health. But in Japan, where most of these infections aren’t endemic, you have to identify rare diseases from among a wide array of other conditions. That means the approach is case-based and individual.
People who are already interested can learn about these topics through sessions like “Learning Tropical Infectious Diseases through Clinical Cases.” But the real goal should be spreading that knowledge to people who aren’t already interested, so they can help recognize rare diseases. That’s something I think about every time I organize a program. On my own, I try to contribute through lectures and talks, quietly but steadily.
Sano:
That makes sense. In endemic settings, diseases affect large populations, so broad public health interventions are needed, but in Japan, the focus is on rare, individual cases.
Nakamura:
From my experiences in Thailand, I actually think their outbreak response system is more advanced than Japan’s. Thailand has multiple administrative levels—village, municipal, district, and provincial. When an outbreak occurs, the upper levels are designed to respond efficiently. If it’s beyond the scope of the local level, a rapid response team is dispatched to investigate and contain the outbreak.
Japan has a similar system on paper, but it doesn’t seem to function as effectively. Thailand borders several countries and constantly faces cross-border infectious threats. After outbreaks of avian flu, SARS, and others, they’ve suffered losses—both in lives and economically—and their system has improved because of those experiences.
Japan, being an island nation, has far fewer infectious disease incursions. That’s why, like we saw during COVID-19, Japan’s healthcare system, which is very individual-centered, struggled when faced with rapid spread. I think that’s a fundamental vulnerability.
Sano:
I had no idea Thailand had such a well-developed system.
Sano:
What kind of work are you currently doing?
Nakamura:
Most of my hospital work is administrative now. Clinically, I still see some outpatients and inpatients, though it’s not a large number. Common cases in the infectious diseases department include urinary tract infections, pneumonia, and aseptic meningitis. Tropical diseases are rare.
Our main treatments involve antimicrobial therapy, but for things like abscess drainage, we request support from other departments. Sometimes we admit patients with fever of unknown origin, and it later turns out to be infective endocarditis (IE). While IE is usually handled by cardiology, if there’s no heart failure or need for surgery, we manage the case within infectious diseases.
Aside from clinical work, I’m often involved in planning training for Category I infectious disease preparedness, and coordinating with outside institutions—Tokyo Metropolitan Government, local public health centers, quarantine stations, and medical associations. Antimicrobial stewardship and infection control are handled by our AST and infection control teams.

Sano:
Right, infectious diseases departments often take the lead on antimicrobial management.
Nakamura:
Bokutoh Hospital originally had an isolation ward for infectious diseases, so treating inpatients with infections is part of its heritage. That’s also why we’re designated as a Category I infectious disease facility, with two Category I beds—meaning we’re equipped to handle the most serious infectious diseases.
Now that the COVID-19 surge has subsided, we need to stay prepared for the next outbreak. Even Ebola virus disease, which is classified as Category I, has become treatable with comprehensive care. In the U.S. and U.K., healthcare workers infected in the field were flown home and survived thanks to intensive treatment.
If something like that were to happen in Japan, we’d have to manage it on an individual basis. That’s why we conduct drills—last year’s training focused on reviewing PPE donning and doffing procedures and patient admission protocols.
Next, we’re planning to train alongside emergency medicine and critical care units, practicing scenarios involving intubation, dialysis, and ventilator use. My job is to ensure our systems are ready and to strengthen coordination with both in-hospital and external partners.
I’m also involved in developing infectious disease response manuals for the Tokyo Metropolitan Government and the Tokyo Metropolitan Hospital Organization. Recently, I was appointed chair of the committee revising the Quick Reference for Infectious Diseases in Inbound Travelers published by the Japanese Association for Infectious Diseases. It’s symptom-based and very user-friendly!
I’m also part of a Ministry of Health research group on Mpox (monkeypox), and I’ve been organizing symposia on tick-borne diseases, which I find fascinating.
*Quick Reference: Approaching Inbound Infectious Diseases from Symptoms Quick Reference on Infectious Diseases
Building Japan’s Future Through Tropical Medicine
Sano:
What do you find most rewarding or exciting about your work now?
Nakamura:
I really enjoy when students who are interested in tropical medicine come to learn. I also find it rewarding to raise awareness about rare tropical diseases at conferences—how to recognize them and what to look for in clinical cases. Sessions like “Learning from Tropical Infectious Disease Cases” let me hear diverse perspectives from colleagues, and that’s fun too.

Sano:
What is the value of Japan—or Japanese people—being involved in tropical medicine?
Nakamura:
The current healthcare system in Japan is very focused on the individual, so I think it’s important to have more people who are interested in public health and large-scale projects. We need to carry on the legacy of those before us who achieved results at the population level.
Personally, I’d really like to see people bring insights from tropical medicine back to Japan—feeding those new perspectives into our domestic systems. That kind of feedback and innovation is essential.
Sano:
What are your goals or dreams for the future?
Nakamura:
I’m beginning to feel the limits of working solely at the individual level. Even while in Japan, I hope to establish a scalable, population-based approach and find ways to communicate it.
Also, I need to hand over the “Learning from Tropical Infectious Disease Cases” session to the next generation soon! (laughs)
Sano:
Finally, do you have any advice or messages for student members of the Tropical Medicine Society?
Nakamura:
Of course, I want to say “keep up the great work!” But beyond that, I really hope you publish papers. Even if your fieldwork is short-term, as long as you’re in the academic world—whether in university or at conferences—you should leave something behind in writing.
A colleague once told me something that stuck with me: “A case report or academic paper is like a commemorative photo.” If you only take a mental snapshot, it’s just a personal memory. But if you publish it, it can trigger responses, open new doors, and contribute to the field.
Publishing may feel daunting, but think of it that way—it helps. And once clinical work starts, it’s easy to get overwhelmed with immediate responsibilities, but I hope everyone keeps their passion for tropical medicine alive.
From left, Yuya Kondo, Dr. Fukumi Nakamura, Haruka Sano
Profile of Interview Participants
Dr. Fukumi Nakamura
Chief, Department of Infectious Diseases, Bokutoh Hospital.
Graduate of Miyazaki Medical College (now University of Miyazaki). While tropical medicine has traditionally focused on research, she contributes from a clinical perspective. At the Japanese Society of Tropical Medicine, she organizes the popular annual workshop “Learning Tropical Medicine through Clinical Cases.” Drawing on her experience during the COVID-19 pandemic, she is also engaged in Category I and II infectious disease preparedness and disaster medicine.
Haruka Sano
Sixth-year medical student, Niigata University School of Medicine.
Originally from Saitama Prefecture. Her interest in tropical medicine and healthcare in low-resource settings began after watching a TV special on Hansen’s disease in junior high school. At university, she is active in the dance club and involved in international exchange. She aspires to become a physician who can contribute to regions with limited access to medical care.

